Despite their ubiquitous presence in the immunological literature, the terms “PBMCs” and “buffy coat” are frequently treated as interchangeable, leading to conceptual ambiguity that may compromise experimental design. As a foundational substrate for vaccine development, immunotherapy, and translational research, precise cellular definition is paramount. This article aims to definitively clarify the biophysical and functional distinctions between these two blood fractions. Furthermore, we provide a systematic overview of current isolation methodologies, empowering researchers to navigate the technical nuances and select the optimal strategy tailored to their specific experimental requirements.
Table of Contents
1. Buffy Coat and PBMCs: definitions, composition, and key differences
2. Principles of PBMC isolation: density gradient centrifugation
3. Comparison of common methods for PBMC isolation
4. Selecting the appropriate PBMC isolation strategy for new laboratories
01 Buffy Coat and PBMCs: definitions, composition, and key differences
Whole blood serves as the primary starting material for immunological analyses, though the actual research focus invariably lies in isolating and characterizing specific target cell subsets. Composed primarily of erythrocytes, leukocytes, platelets, and plasma, whole blood sees its plasma fraction rich in water, albumin, coagulation factors, and various soluble components. Leukocytes are broadly categorized into two major lineages: peripheral blood mononuclear cells (PBMCs) and polymorphonuclear cells (PMNs, commonly referred to as granulocytes).
Freshly collected anticoagulated whole blood is centrifuged at 800-1000 × g for 10–15 minutes, resulting in the natural separation of three distinct layers (Fig. 1). The upper layer (~55% of total volume) consists of pale-yellow, translucent plasma. The bottom layer (~45%) comprises a dark red pellet of erythrocytes, often containing minor granulocyte contaminants. Sandwiched between these layers is a thin, grayish-white interface known as the buffy coat, which accounts for less than 1% of the total volume. This leukocyte-platelet concentrate contains granulocytes, mononuclear cells, platelets, and residual red blood cells. Owing to substantial interference from contaminating granulocytes and platelets, the buffy coat is unsuitable for direct use in most immunological functional experiments, such as T cell functional analysis, monocyte differentiation, and PBMC transcriptomics.
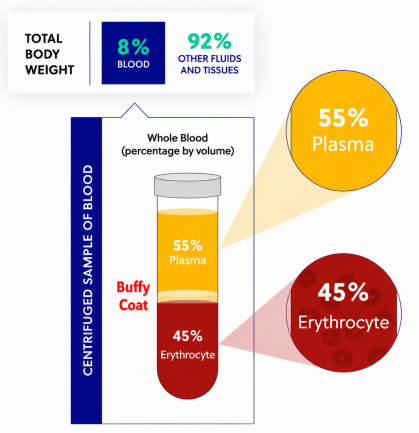
Fig. 1 Centrifuged sample of blood.
To obtain a purified population free of these contaminants, PBMCs are isolated from whole blood or the buffy coat via density gradient centrifugation using Ficoll or similar media. By definition, PBMCs specifically refer to all peripheral blood cells possessing a single, rounded nucleus, primarily lymphocytes and monocytes, while polymorphonuclear granulocytes and the vast majority of erythrocytes are effectively removed. Therefore, it is crucial to emphasize that “PBMCs” and “buffy coat” are not interchangeable terms: the former is a crude, mixed cell layer obtained directly after whole blood centrifugation, whereas the latter is a refined mononuclear cell fraction purified through density gradient centrifugation.
02 Principles of PBMC isolation: density gradient centrifugation
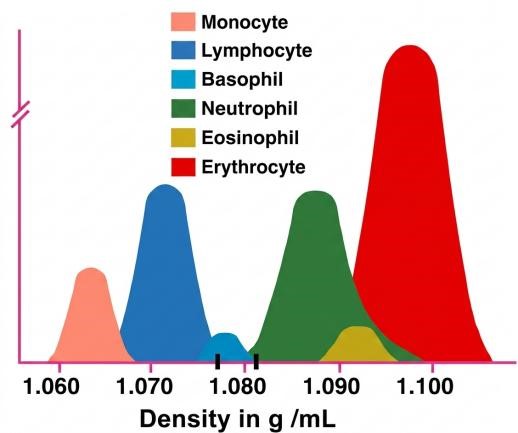
Fig. 2 Density of various visible components in human blood.
The fundamental principle underlying PBMC isolation relies on differential buoyant densities among blood cell populations. Ficoll-Hypaque separation medium is formulated to a density of 1.077 g/mL, serving as a buoyant density barrier positioned between granulocytes and mononuclear cells. When diluted blood is carefully layered over the medium and centrifuged, erythrocytes and granulocytes (density >1.077 g/mL) pellet at the bottom, while PBMCs (density <1.077 g/mL) are retained at the plasma-Ficoll interface, forming a distinct, cloudy white band. Platelets, being lighter still, largely remain suspended in the upper plasma layer, with only minimal contamination of the PBMC band[1,2].
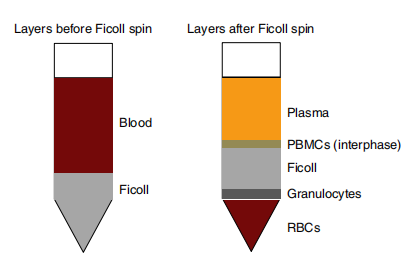
Fig. 3 Ficoll density gradient of leukopac for the separation of PBMCs. PBMCs are enriched in the interphase between plasma and Ficoll layers, whereas granulocytes and red blood cells (RBCs) are pelleted[3].
03 Comparison of common methods for PBMC isolation
3.1 Density Gradient Centrifugation (The Ficoll Method)
This is the most classic and widely cited method for isolating mononuclear cells from peripheral or cord blood, relying on Ficoll-Hypaque density gradient centrifugation with a density of 1.077 g/mL. Ficoll, a high-molecular-weight sucrose polymer, contributes viscosity and promotes rouleaux formation of erythrocytes, whereas Hypaque (sodium diatrizoate) increases the solution’s density. The approach offers several advantages, including cost-effectiveness, reliability, rapid processing, and minimal alteration of cell phenotype or function. Typical yields from healthy donors range from 1-2 × 106 mononuclear cells per milliliter of blood, with viability exceeding 95%[3,4].
However, the protocol is labor-intensive, requiring careful layering of diluted blood over or under the Ficoll-Hypaque solution and precise control of centrifugation conditions (e.g., 900 × g for 20-30 minutes at 18-20°C) to prevent interface disturbance. A critical yet often overlooked detail: always turn off the centrifuge brake ( “Brake Off” ) and allow the rotor to coast to a stop. The cell layers formed on a Ficoll gradient are surprisingly delicate; abrupt deceleration from a braked stop can generate enough turbulence to disrupt the sharp interface, leading to poor separation and loss of the mononuclear cell band[4].
3.2 CPT Tubes (Ready-to-Use Cell Preparation Tubes)
The Vacutainer CPT (Cell Preparation Tube) integrates sodium citrate anticoagulant, a Ficoll-based density medium, and a thixotropic polyester gel. During centrifugation, the gel flows and then solidifies between the high-density cells (granulocytes and erythrocytes) and the PBMC layer, creating a stable physical barrier that prevents remixing of cell populations. Consequently, PBMCs are securely lodged at the interface above the gel and below the plasma, as described by Corkum et al[5].
This design greatly simplifies the workflow: there is no need to manually layer blood over a density medium or to open tubes during processing. The CPT method minimizes technical variability, reduces cell handling, and shortens processing time, making it particularly advantageous for large-scale clinical studies. According to Corkum et al[5], the mean yield and viability of PBMCs isolated by CPT (1.34 × 106 cells/mL, 93.3 %) are comparable to those obtained by conventional Ficoll-Paque gradient centrifugation (1.16 × 106 cells/mL, 97.2%). Moreover, the CPT protocol does not adversely affect the purity, recovery, or gene expression profiles of downstream immune cell subsets (CD19+ B cells, CD4+ and CD8+ T cells, and CD14+ monocytes).
However, the CPT system has a notable drawback: each tube costs considerably more than a standard Ficoll setup, making it less economical for routine or large-volume preparations. Additionally, the manufacturer notes that CPT-isolated PBMC may show higher red blood cell contamination, often requiring an extra lysis step.
3.3 SepMate Tubes
The defining feature of a SepMate tube is the porous plastic insert inside. It physically separates the blood from the density medium (Lymphoprep) before centrifugation. When the run starts, the diluted blood must pass through the pores of the insert to reach the Lymphoprep layer. This design prevents the two liquid phases from mixing during loading and yields an exceptionally clean interface without the need for careful layering.
According to Grievink et al[6], SepMate tubes offer several clear practical advantages. PBMC recovery is approximately 70% higher than with classic Ficoll-Paque centrifugation (8 × 105 vs. 6 × 105 cells per mL of whole blood). The procedure is straightforward: after a single centrifugation step (1,200 × g for 10 minutes with brake on), PBMCs can be simply poured off, reducing operator-to-operator variability and processing time. Cell viability remains excellent (close to 100 % by trypan blue exclusion), and the composition of major immune subsets (T cells, B cells, NK cells, monocytes) does not differ significantly from Ficoll-isolated preparations.
However, the study also noted that SepMate-isolated PBMCs produced higher spontaneous cytokine release (e.g., IL-6 and IL-8) and stronger SEB-induced IFN-γ and secondary cytokine responses compared to Ficoll-isolated cells. This may reflect subtle cell activation due to the isolation procedure, which could confound certain functional assays. A similar trend was observed for CPT (Cell Preparation Tube) isolation[5], which gave the highest cell recovery (13 × 105 cells/mL) but also the most pronounced spontaneous cytokine release and red blood cell contamination.
3.4 Immunomagnetic Bead-Based Sorting
If you do not need the full PBMC population but are after a specific subset (e.g., CD3+ T cells), you can label the target cells directly in blood with magnetic beads and pull them out in a magnetic field. Negative-selection kits that deplete all unwanted cells (platelets, granulocytes, erythrocytes) while leaving your cells of interest untouched are also available. As described by Villalva et al[7], this negative-selection approach uses an antibody cocktail against unwanted populations, followed by magnetic removal, allowing recovery of purified lymphocytes and monocytes directly from the buffy coat without prior density gradient centrifugation.
The strength of negative-selection approach is its exceptionally high purity and preserved cell functionality, since the target cells are never bound by antibodies or beads. It is also highly scalable: the same kit can be used for manual processing (up to 8 samples with a simple magnet stand) or fully automated processing (using a dedicated instrument), making it suitable for high-throughput biobanking. Villalva et al. reported that PBMCs isolated by negative magnetic separation showed comparable viability (>95 %), population composition (lymphocytes, monocytes), and recovery to those obtained by density gradient centrifugation[7].
3.5 Automated Cell Separation Instruments
Devices such as Sepax and CliniMACS are used mainly for clinical-grade, GMP-compliant large-scale production. The whole sequence (liquid addition, centrifugation, fraction collection) is performed automatically inside a closed system. The degree of standardization is impeccable, but the upfront cost of the equipment and the consumables is so high that these instruments are usually beyond the reach of a newly established small lab.
04 Selecting the appropriate PBMC isolation strategy for new laboratories
If you are just setting up your lab, or still getting a feel for these techniques, I would strongly suggest starting with Ficoll density gradient centrifugation.
This is not because the other methods are inadequate, but because the Ficoll method is uniquely suited to the early stages of a project. It keeps costs to a bare minimum: Ficoll medium is inexpensive and works perfectly well with standard centrifuge tubes and pipettes, and that financial latitude is invaluable when you need to run a lot of preliminary experiments to dial in your conditions.
Even more important, it gives you genuine hands-on experience with cell isolation. Diluting the blood yourself, slowly layering it, carefully collecting the whitish band, every round of this process builds an intuitive feel for cell densities, viscosity, and the effect of centrifugal force. The muscle memory you develop will deepen your understanding of the separation principle far more than pushing a button ever could.
And when a tricky sample comes along, cord blood or bone marrow, for instance, the buffer ratios and centrifugation parameters of the Ficoll method can be fine-tuned on the fly. Closed commercial tube systems rarely offer that kind of flexibility; when something goes wrong, you often have no choice but to discard the tube and start over.
A few practical details are easy to overlook but frequently make or break the result, so it is worth building them into your routine from the start:
(1) Work at room temperature throughout. Cold temperatures promote cell clumping, which does more harm than good.
(2) Always centrifuge with the brake off, letting the rotor decelerate naturally. An abrupt stop can churn the interface and undo all the care you took during layering.
(3) When aspirating the PBMC band, use a light touch. It is better to leave a little behind than to contaminate your cells with red blood cells from the pellet.
PBMCs are the starting material for countless immunological experiments, and Ficoll density gradient centrifugation is the first real technical threshold a new lab needs to cross. Once you have this step down, the cell-based experiments that follow will feel much smoother. With consistent technique, you can routinely obtain PBMC preparations with high yield, purity, and viability.
References:
[1] MBöyum A. Separation of leukocytes from blood and bone marrow. Introduction. Scand J Clin Lab Invest Suppl. 1968;97:7.
[2] Ulmer AJ, Scholz W, Ernst M, Brandt E, Flad HD. Isolation and subfractionation of human peripheral blood mononuclear cells (PBMC) by density gradient centrifugation on Percoll. Immunobiology. 1984;166(3):238-250.
[3] Lin Z, Chiang NY, Chai N, et al. In vivo antigen-driven plasmablast enrichment in combination with antigen-specific cell sorting to facilitate the isolation of rare monoclonal antibodies from human B cells. Nat Protoc. 2014;9(7):1563-1577.
[4] Fuss IJ, Kanof ME, Smith PD, Zola H. Isolation of whole mononuclear cells from peripheral blood and cord blood. Curr Protoc Immunol. 2009;Chapter 7:7.1.1-7.1.8. doi:10.1002/0471142735.im0701s85
[5] Corkum CP, Ings DP, Burgess C, Karwowska S, Kroll W, Michalak TI. Immune cell subsets and their gene expression profiles from human PBMC isolated by Vacutainer Cell Preparation Tube (CPT™) and standard density gradient. BMC Immunol. 2015;16:48. Published 2015 Aug 26.
[6] Grievink HW, Luisman T, Kluft C, Moerland M, Malone KE. Comparison of Three Isolation Techniques for Human Peripheral Blood Mononuclear Cells: Cell Recovery and Viability, Population Composition, and Cell Functionality. Biopreserv Biobank. 2016;14(5):410-415.
[7] Villalva M, Macphail S, Li Y, Caruana B. Isolating Human Peripheral Blood Mononuclear Cells from Buffy Coats via High Throughput Immunomagnetic Bead Separation. J Vis Exp. 2024;(209):10.3791/66887. Published 2024 Jul 19.

